Dextroamphetamine Saccharate, Amphetamine Aspartate Monohydrate, Dextroamphetamine Sulfate, and Amphetamine Sulfate
ORAL
Dextroamphetamine Saccharate, Amphetamine Aspartate Monohydrate, Dextroamphetamine Sulfate, and Amphetamine Sulfate. INDICATIONS AND USAGE Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-rel
Boxed warning
WARNING: ABUSE, MISUSE, and ADDICTION Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules have a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules, can result in overdose and death [see Overdosage ( 10 )] , and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection. Before prescribing dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug. Throughout dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction [see Warnings and Precautions ( 5.1 ), Drug Abuse and Dependence ( 9.2 )]. WARNING: ABUSE, MISUSE, and ADDICTION See full prescribing information for complete boxed warning Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules have a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules, can result in overdose and death ( 5.1 , 9.2 , 10 ) • Before prescribing dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules, assess each patient’s risk for abuse, misuse, and addiction. • Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug. • Throughout treatment, reassess each patient’s risk and frequently monitor for signs and symptoms of abuse, misuse, and addiction.
Brand names
Dextroamphetamine Saccharate, Amphetamine Aspartate Monohydrate, Dextroamphetamine Sulfate, and Amphetamine SulfateDextroamphetamine Saccharate, Amphetamine Aspartate Monohydrate, Dextroamphetamine Sulfate and Amphetamine SulfateDEXTROAMPHETAMINE SACCHARATE, AMPHETAMINE ASPARTATE MONOHYDRATE, DEXTROAMPHETAMINE SULFATE AND AMPHETAMINE SULFATEdextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfateDextroamphetamine Saccharate, Amphetamine Aspartate Monohydrate, Dextroamphetamine Sulfate, and Amphetamine Sulfate Extended-ReleaseDextroamphetamine Saccharate, Amphetamine Aspartate, Dextroamphetamine Sulfate, and Amphetamine Sulfatedextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate
INDICATIONS AND USAGE Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules, a CNS stimulant, are indicated for the treatment of attention deficit hyperactivity disorder (ADHD). ( 1 ) • Children (ages 6-12): Efficacy was established in one 3-week outpatient, controlled trial and one analogue classroom, controlled trial in children with ADHD. ( 14 ) • Adolescents (ages 13-17): Efficacy was established in one 4-week controlled trial in adolescents with ADHD. ( 14 ) • Adults: Efficacy was established in one 4-week controlled trial in adults with ADHD. ( 14 ) 1.1 Attention Deficit Hyperactivity Disorder Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules are indicated for the treatment of attention deficit hyperactivity disorder (ADHD). The efficacy of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules in the treatment of ADHD was established on the basis of two controlled trials in children aged 6 to 12, one controlled trial in adolescents aged 13 to 17, and one controlled trial in adults who met DSM-IV ® criteria for ADHD [see Clinical Studies ( 14 )] . A diagnosis of ADHD (DSM-IV ® ) implies the presence of hyperactive-impulsive or inattentive symptoms that caused impairment and were present before age 7 years. The symptoms must cause clinically significant impairment, e.g., in social, academic, or occupational functioning, and be present in two or more settings, e.g., school (or work) and at home. The symptoms must not be better accounted for by another mental disorder. For the Inattentive Type, at least six of the following symptoms must have persisted for at least 6 months: lack of attention to details/careless mistakes; lack of sustained attention; poor listener; failure to follow through on tasks; poor organization; avoids tasks requiring sustained mental effort; loses things; easily distracted; forgetful. For the Hyperactive-Impulsive Type, at least six of the following symptoms must have persisted for at least 6 months: fidgeting/squirming; leaving seat; inappropriate running/climbing; difficulty with quiet activities; "on the go;" excessive talking; blurting answers; can't wait turn; intrusive. The Combined Type requires both inattentive and hyperactive-impulsive criteria to be met. Special Diagnostic Considerations Specific etiology of this syndrome is unknown, and there is no single diagnostic test. Adequate diagnosis requires the use not only of medical but of special psychological, educational, and social resources. Learning may or may not be impaired. The diagnosis must be based upon a complete history and evaluation of the patient and not solely on the presence of the required number of DSM-IV ® characteristics. Need for Comprehensive Treatment Program Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules are indicated as an integral part of a total treatment program for ADHD that may include other measures (psychological, educational, social) for patients with this syndrome. Drug treatment may not be indicated for all patients with this syndrome. Stimulants are not intended for use in the patient who exhibits symptoms secondary to environmental factors and/or other primary psychiatric disorders, including psychosis. Appropriate educational placement is essential and psychosocial intervention is often helpful. When remedial measures alone are insufficient, the decision to prescribe stimulant medication will depend upon the physician's assessment of the chronicity and severity of the child's symptoms. Long-Term Use The effectiveness of dextroamphetamine sulfate, dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules for long-term use, i.e., for more than 3 weeks in children and 4 weeks in adolescents and adults, has not been systematically evaluated in controlled trials. Therefore, the physician who elects to use dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules for extended periods should periodically re-evaluate the long-term usefulness of the drug for the individual patient.
Dosage
DOSAGE AND ADMINISTRATION Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules should be administered once daily upon awakening. Recommended Starting Dose Titration Schedule Maximum Daily Dose Adults 12.5 mg 12.5 mg weekly 50 mg Pediatrics (13 to 17) 12.5 mg 12.5 mg weekly 25 mg In adult patients with severe renal impairment the maximum dose should not exceed 25 mg daily. Use in adult patients with ESRD is not recommended. ( 2.6 , 8.6 ) The maximum dose in pediatric patients with severe renal impairment is 12.5 mg daily. Use in pediatric patients with ESRD is not recommended. ( 2.6 , 8.6 ) Patients are advised to take consistently either with or without food. ( 2.2 ) Administer upon awakening because the effects may last up to 16 hours and there is the potential for insomnia. ( 2.2 ) Prior to treatment, assess for presence of cardiac disease. ( 2.1 ) To avoid substitution errors and overdosage, do not substitute for other amphetamine products on a milligram-per-milligram basis because of different amphetamine base compositions and differing pharmacokinetic profiles. ( 2.7 ) 2.1 Pretreatment Screening Prior to treating patients with dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules, assess: for the presence of cardiac disease (i.e., perform a careful history, family history of sudden death or ventricular arrhythmia, and physical exam) [see Warnings and Precautions ( 5.2 )] the family history and clinically evaluate patients for motor or verbal tics or Tourette’s syndrome before initiating dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules [see Warnings and Precautions ( 5.10 )] 2.2 General Administration Information Because the effects of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules may last up to 16 hours and there is potential for insomnia, administer once daily in the morning upon awakening. In the event of a missed dose, do not administer later in the day. Do not administer additional medication to make up for the missed dose [see Adverse Reactions ( 6.1 ), Clinical Studies ( 14 )]. 2.3 Administration Instructions Administer dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules orally with or without food. Advise patients to take dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules consistently either with food or without food [see Clinical Pharmacology ( 12.3 )]. Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules may be administered in one of the following ways: Swallow dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules whole, or Open capsule and sprinkle the entire contents over a spoonful of applesauce. The sprinkled applesauce should be consumed immediately; it should not be stored. Patients should take the sprinkled applesauce in its entirety without chewing. The dose of a single capsule should not be divided. 2.4 Recommended Dosage Adults (18 to 55 years) The recommended starting dose of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules is 12.5 mg once daily in the morning upon awakening. Initial doses of 25 mg once daily may be considered for some patients. Dosage may be adjusted in increments of 12.5 mg no sooner than weekly, up to a maximum dose of 50 mg once daily, based on the therapeutic needs and response of the patient. Doses above 50 mg daily have shown no additional clinically meaningful benefit. Pediatric Patients (13 to 17 years) The recommended starting dose is 12.5 mg once daily in the morning upon awakening. Dosage may be adjusted in increments of 12.5 mg no sooner than weekly, up to a recommended maximum dose of 25 mg once daily. The dose should be individualized according to the needs and response of the patient. Doses higher than 25 mg have not been evaluated in clinical trials in pediatric patients. 2.5 Dosage Modifications Due to Drug Interactions Agents that alter gastrointestinal and urinary pH can impact urinary excretion and alter blood levels of amphetamine. Acidifying agents (e.g., ascorbic acid) decrease blood levels, while alkalinizing agents (e.g., sodium bicarbonate) increase blood levels. Adjust dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsule dosage accordingly [see Drug Interactions ( 7.1 )]. 2.6 Dosage in Patients with Renal Impairment In adult patients with severe renal impairment (GFR between 15 to <30 mL/min/1.73 m 2 ), the recommended starting dose of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules is 12.5 mg daily with a maximum recommended dose of 25 mg daily. Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules are not recommended for use in patients with end stage renal disease (ESRD <15 mL/min/1.73 m 2 ). In pediatric patients (13 to 17 years) with severe renal impairment, the maximum dose is 12.5 mg, if tolerated [see Use in Specific Populations ( 8.6 ), Clinical Pharmacology ( 12.3 )]. 2.7 Switching From Other Amphetamine Products For patients switching from another medication or any other amphetamine products, discontinue that treatment, and titrate with dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules using the titration schedule [see Dosage and Administration (2.4) ] . Do not substitute for other amphetamine products on a milligram-per-milligram basis because of different amphetamine base compositions and differing pharmacokinetic profiles [see Warnings and Precautions ( 5.9 ), Description ( 11 ), Clinical Pharmacology ( 12.3 )].
Warnings
WARNINGS AND PRECAUTIONS Risks to Patients with Serious Cardiac Disease: Avoid use in patients with known structural cardiac abnormalities, cardiomyopathy, serious cardiac arrhythmias, coronary artery disease, or other serious cardiac disease. ( 5.2 ) Increased Blood Pressure and Heart Rate: Monitor blood pressure and pulse at appropriate intervals. ( 5.3 ) Psychiatric Adverse Reactions: Prior to initiating dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules, screen patients for risk factors for developing a manic episode. If new psychotic or manic symptoms occur, consider discontinuing dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules. ( 5.4 ) Long-Term Suppression of Growth in Pediatric Patients: Closely monitor growth (height and weight) in pediatric patients. Pediatric patients not growing or gaining height or weight as expected may need to have their treatment interrupted. ( 5.5 ) Seizures: May lower the convulsive threshold. Discontinue in the presence of seizures. ( 5.6 ) Peripheral Vasculopathy, including Raynaud's phenomenon: Stimulants used to treat ADHD are associated with peripheral vasculopathy, including Raynaud's Phenomenon: Careful observation for digital changes is necessary during dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules treatment. Further clinical evaluation (e.g., rheumatology referral) may be appropriate for patients who develop signs or symptoms of peripheral vasculopathy. ( 5.7 ) Serotonin Syndrome: Increased risk when co-administered with serotonergic agents (e.g., SSRIs, SNRIs, triptans), but also during overdosage situations. If it occurs, discontinue dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules and initiate supportive treatment ( 4 , 5.8 , 10 ). Motor and Verbal Tics, and Worsening of Tourette's Syndrome: Before initiating dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules, assess the family history and clinically evaluate patients for tics or Tourette's syndrome. Regularly monitor patients for the emergence or worsening of tics or Tourette's syndrome. Discontinue treatment if clinically appropriate. ( 5.9 ) 5.1 Abuse, Misuse, and Addiction Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules have a high potential for abuse and misuse. The use of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules exposes individuals to the risks of abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules can be diverted for non-medical use into illicit channels or distribution [see Drug Abuse and Dependence (9.2) ] . Misuse and abuse of CNS stimulants, including dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules, can result in overdose and death [see Overdosage (10) ] , and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection. Before prescribing dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks and proper disposal of any unused drug. Advise patients to store dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules in a safe place, preferably locked, and instruct patients to not give dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules to anyone else. Throughout dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction. 5.2 Risks to Patients with Serious Cardiac Disease Sudden death has been reported in patients with structural cardiac abnormalities or other serious cardiac disease who were treated with CNS stimulants at the recommended ADHD dosage. Avoid dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules use in patients with known structural cardiac abnormalities, cardiomyopathy, serious cardiac arrhythmia, coronary artery disease, or other serious cardiac disease. 5.3 Increased Blood Pressure and Heart Rate CNS stimulants may cause an increase in blood pressure (mean increase approximately 2 to 4 mmHg) and heart rate (mean increase approximately 3 to 6 bpm). Monitor all dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules treated patients for hypertension and tachycardia. 5.4 Psychiatric Adverse Reactions Exacerbation of Pre-Existing Psychosis Administration of stimulants may exacerbate symptoms of behavior disturbance and thought disorder in patients with pre-existing psychotic disorder. Induction of a Manic Episode in Patients with Bipolar Disease CNS stimulants may induce a manic or mixed episode in patients. Prior to initiating dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules treatment, screen patients for risk factors for developing a manic episode (e.g., comorbid or history of depressive symptoms or a family history of suicide, bipolar disorder, and depression). New Psychotic or Manic Symptoms CNS stimulants, at the recommended dosage, may cause psychotic or manic symptoms, (e.g., hallucinations, delusional thinking, or mania) in patients without a prior history of psychotic illness or mania. In a pooled analysis of multiple short- term, placebo-controlled studies of CNS stimulants, psychotic or manic symptoms occurred in approximately 0.1% of CNS stimulant-treated patients compared to 0% of placebo-treated patients. If such symptoms occur, consider discontinuing dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules. 5.5 Long-Term Suppression of Growth in Pediatric Patients Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules is not approved for use and is not recommended in pediatric patients below 6 years of age [see Use in Specific Populations (8.4) ] . CNS stimulants have been associated with weight loss and slowing of growth rate in pediatric patients. Closely monitor growth (weight and height) in dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules-treated pediatric patients treated with CNS stimulants. In a controlled trial of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules in adolescents, mean weight change from baseline within the initial 4 weeks of therapy was -1.1 lbs. and -2.8 lbs., respectively, for patients receiving 10 mg and 20 mg dextroamphe
Contraindications
CONTRAINDICATIONS Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsule administration is contraindicated in patients with the following conditions: • Advanced arteriosclerosis • Symptomatic cardiovascular disease • Moderate to severe hypertension • Hyperthyroidism • In patients known to be hypersensitive to amphetamine, or other components of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules. Hypersensitivity reactions such as angioedema and anaphylactic reactions have been reported in patients treated with other amphetamine products [see Adverse Reactions ( 6.2 )] • Glaucoma • Agitated states • History of drug abuse • Patients taking monoamine oxidase inhibitors (MAOIs), or within 14 days of stopping MAOIs (including MAOIs such as linezolid or intravenous methylene blue), because of an increased risk of hypertensive crisis [see Warnings and Precautions ( 5.6 ) and Drug Interactions ( 7.1 )] • Advanced arteriosclerosis ( 4 ) • Symptomatic cardiovascular disease ( 4 ) • Moderate to severe hypertension ( 4 ) • Hyperthyroidism ( 4 ) • Known hypersensitivity or idiosyncrasy to amphetamine ( 4 ) • Glaucoma ( 4 ) • Agitated states ( 4 ) • History of drug abuse ( 4 ) • During or within 14 days following the administration of monoamine oxidase inhibitors (MAOI) ( 4 , 7.1 )
Drug interactions
DRUG INTERACTIONS • MAOI antidepressants are contraindicated; MAOIs potentiate the effects of amphetamine. Do not administer dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules during or within 14 days after use of MAOI. ( 4 , 7.1 ). • Alkalinizing agents (GI antacids and urinary): These agents increase blood levels of amphetamine. ( 7.1 ) • Acidifying agents (GI and urinary): These agents reduce blood levels of amphetamine. ( 7.1 ) • Adrenergic blockers, antihistamines, antihypertensives, phenobarbital, phenytoin, veratrum alkaloids, and ethosuximide: Effects may be reduced by amphetamines. ( 7.1 ) • Tricyclic antidepressants, norepinephrine, and meperidine: Effects may be potentiated by amphetamines. ( 7.1 ) 7.1 Clinically Important Interactions with Amphetamines Table 4: Drugs Having Clinically Important Interactions with Amphetamines Monoamine Oxidase Inhibitors (MAOIs) Clinical Impact Concomitant use of MAOIs and CNS stimulants can cause hypertensive crisis. Potential outcomes include death, stroke, myocardial infarction, aortic dissection, ophthalmological complications, eclampsia, pulmonary edema, and renal failure. Intervention Do not administer dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules concomitantly or within 14 days after discontinuing MAOI [see Contraindications ( 4 )]. Examples selegiline, tranylcypromine, isocarboxazid, phenelzine, linezolid, methylene blue Serotonergic Drugs Clinical Impact The concomitant use of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules and serotonergic drugs increases the risk of serotonin syndrome. Intervention Initiate with lower doses and monitor patients for signs and symptoms of serotonin syndrome, particularly during dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsule initiation or dosage increase. If serotonin syndrome occurs, discontinue dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules and the concomitant serotonergic drug(s) [see Warnings and Precautions ( 5.6 )]. Examples selective serotonin reuptake inhibitors (SSRI), serotonin norepinephrine reuptake inhibitors (SNRI), triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, St. John’s Wort CYP2D6 Inhibitors Clinical Impact The concomitant use of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules and CYP2D6 inhibitors may increase the exposure of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules compared to the use of the drug alone and increase the risk of serotonin syndrome. Intervention Initiate with lower doses and monitor patients for signs and symptoms of serotonin syndrome particularly during dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsule initiation and after a dosage increase. If serotonin syndrome occurs, discontinue dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules and the CYP2D6 inhibitor [see Warnings and Precautions ( 5.6 ) and Overdosage ( 10 )]. Examples paroxetine and fluoxetine (also serotonergic drugs), quinidine, ritonavir Alkalinizing Agents Clinical Impact Increase blood levels and potentiate the action of amphetamine. Intervention Co-administration of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate, and amphetamine sulfate extended-release capsules and gastrointestinal or urinary alkalinizing agents should be avoided. Examples Gastrointestinal alkalinizing agents (e.g., sodium bicarbonate). Urinary alkalinizing agents (e.g., acetazolamide, some thiazides). Acidifying Agents Clinical Impact Lower blood levels and efficacy of amphetamines. Intervention Increase dose based on clinical response. Examples Gastrointestinal acidifying agents (e.g., guanethidine, reserpine, glutamic acid HCl, ascorbic acid). Urinary acidifying agents (e.g., ammonium chloride, sodium acid phosphate, methenamine salts). Tricyclic Antidepressants Clinical Impact May enhance the activity of tricyclic or sympathomimetic agents causing striking and sustained increases in the concentration of d-amphetamine in the brain; cardiovascular effects can be potentiated. Intervention Monitor frequently and adjust or use alternative therapy based on clinical response. Examples desipramine, protriptyline Proton Pump Inhibitors Clinical Impact Time to maximum concentration (T max ) of amphetamine is decreased compared to when administered alone. Intervention Monitor patients for changes in clinical effect and adjust therapy based on clinical response. Examples Omeprazole
Adverse reactions
ADVERSE REACTIONS The following adverse reactions are discussed in greater detail in other sections of the labeling: Abuse, Misuse, and Addiction [see Boxed Warning, Warnings and Precautions (5.1) , Drug Abuse and Dependence (9.2, 9.3 )] Risks to Patients with Serious Cardiac Disease [see Warnings and Precautions (5.2) ] Increased Blood Pressure and Heart Rate [see Warnings and Precautions (5.3) ] Psychiatric Adverse Reactions [see Warnings and Precautions (5.4) ] Long-Term Suppression of Growth in Pediatric Patients [see Warnings and Precautions (5.5) ] Seizures [see Warnings and Precautions (5.6) ] Peripheral Vasculopathy, including Raynaud’s Phenomenon [see Warnings and Precautions (5.7) ] Serotonin Syndrome [see Warnings and Precautions (5.8) ] Motor and Verbal Tics, and Worsening of Tourette’s Syndrome [see Warnings and Precautions (5.9) ] Pediatric patients ages 6 to 12: Most common adverse reactions (≥5% and with a higher incidence than on placebo) were loss of appetite, insomnia, abdominal pain, emotional lability, vomiting, nervousness, nausea, and fever. (6.1) Pediatric patients ages 13 to 17: Most common adverse reactions (≥5% and with a higher incidence than on placebo) were loss of appetite, insomnia, abdominal pain, weight loss, and nervousness. (6.1) Adults: Most common adverse reactions ≥5% and with a higher incidence than on placebo were dry mouth, loss of appetite, insomnia, headache, weight loss, nausea, anxiety, agitation, dizziness, tachycardia, diarrhea, asthenia, and urinary tract infections. (6.1) To report SUSPECTED ADVERSE REACTIONS, contact Elite Laboratories, Inc. at 1-888-852-6657 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch 6.1 Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The premarketing development program for dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules included exposures in a total of 1,315 participants in clinical trials (635 pediatric patients, 350 adolescent patients, 248 adult patients, and 82 healthy adult subjects). Of these, 635 patients (ages 6 to 12) were evaluated in two controlled clinical studies, one open-label clinical study, and two single-dose clinical pharmacology studies (N= 40). Safety data on all patients are included in the discussion that follows. Adverse reactions were assessed by collecting adverse reactions, results of physical examinations, vital signs, weights, laboratory analyses, and ECGs. Adverse reactions during exposure were obtained primarily by general inquiry and recorded by clinical investigators using terminology of their own choosing. Consequently, it is not possible to provide a meaningful estimate of the proportion of individuals experiencing adverse reactions without first grouping similar types of reactions into a smaller number of standardized event categories. In the tables and listings that follow, COSTART terminology has been used to classify reported adverse reactions. The stated frequencies of adverse reactions represent the proportion of individuals who experienced, at least once, a treatment-emergent adverse event of the type listed. Adverse Reactions Leading to Discontinuation of Treatment In two placebo-controlled studies of up to 5 weeks duration among children with ADHD, 2.4% (10/425) of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsule-treated patients discontinued due to adverse reactions (including three patients with loss of appetite, one of whom also reported insomnia) compared to 2.7% (7/259) receiving placebo. The most frequent adverse reactions leading to discontinuation of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules in controlled and uncontrolled, multiple-dose clinical trials of children (N=595) were anorexia (loss of appetite) (2.9%), insomnia (1.5%), weight loss (1.2%), emotional lability (1%), and depression (0.7%). Over half of these patients were exposed to dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules for 12 months or more. In a separate placebo-controlled 4-week study in adolescents with ADHD, five patients (2.1%) discontinued treatment due to adverse events among dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsule-treated patients (N=233) compared to none who received placebo (N=54). The most frequent adverse event leading to discontinuation and considered to be drug-related (i.e., leading to discontinuation in at least 1% of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsule-treated patients and at a rate at least twice that of placebo) was insomnia (1.3%, n=3). In one placebo-controlled 4 week study among adults with ADHD with doses 20 to 60 mg, 23 patients (12.0%) discontinued treatment due to adverse events among dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsule-treated patients (N=191) compared to one patient (1.6%) who received placebo (N=64). The most frequent adverse events leading to discontinuation and considered to be drug-related (i.e., leading to discontinuation in at least 1% of dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsule-treated patients and at a rate at least twice that of placebo) were insomnia (5.2%, n=10), anxiety (2.1%, n=4), nervousness (1.6%, n=3), dry mouth (1.6%, n=3), anorexia (1.6%, n=3), tachycardia (1.6%, n=3), headache (1.6%, n=3), and asthenia (1.0%, n=2). Adverse Reactions Occurring in Controlled Trials Adverse reactions reported in a 3 week clinical trial of children and a 4 week clinical trial in adolescents and adults, respectively, treated with dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules or placebo are presented in the tables below. Table 1: Adverse Reactions Reported by 2% or More of Children (6 to 12 Years Old) Receiving Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules with Higher Incidence Than on Placebo in a 584 Patient Clinical Study Body System Preferred Term Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules (n=374) Placebo (n=210) General Abdominal Pain (stomachache) Fever Infection Accidental Injury Asthenia (fatigue) 14% 5% 4% 3% 2% 10% 2% 2% 2% 0% Digestive System Loss of Appetite Vomiting Nausea Dyspepsia 22% 7% 5% 2% 2% 4% 3% 1% Nervous System Insomnia Emotional Lability Nervousness Dizziness 17% 9% 6% 2% 2% 2% 2% 0% Metabolic/ Nutritional Weight Loss 4% 0% Table 2: Adverse Reactions Reported by 5% or More of Adolescents (13 to 17 Years Old) Weighing ≤ 75 kg/165 lbs Receiving Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules with Higher Incidence Than Placebo in a 287 Patient Clinical Forced Weekly-Dose Titration Study* Body System Preferred Term Dextroamphetamine saccharate, amphetamine aspartate monohydrate, dextroamphetamine sulfate and amphetamine sulfate extended-release capsules (n=233) Placebo (n=54) General Abdominal Pain (stomachache) 11% 2% Digestive S
Mechanism of action
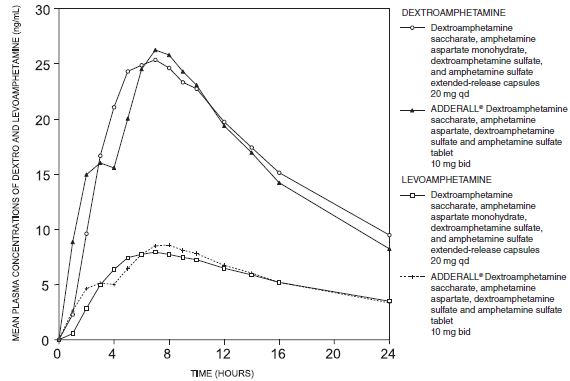
CLINICAL PHARMACOLOGY Pharmacodynamics Amphetamines are non-catecholamine sympathomimetic amines with CNS stimulant activity. The mode of therapeutic action in Attention Deficit Hyperactivity Disorder (ADHD) is not known. Amphetamines are thought to block the reuptake of norepinephrine and dopamine into the presynaptic neuron and increase the release of these monoamines into the extraneuronal space. Pharmacokinetics Mixed salts of a single entity amphetamine product contain d-amphetamine and l-amphetamine salts in the ratio of 3:1. Following administration of a single dose 10 mg or 30 mg of mixed salts of a single entity amphetamine product to healthy volunteers under fasted conditions, peak plasma concentrations occurred approximately 3 hours post-dose for both d-amphetamine and l-amphetamine. The mean elimination half‑life (t ½ ) for d-amphetamine was shorter than the t ½ of the l-isomer (9.77 to 11 hours vs. 11.5 to 13.8 hours). The PK parameters (C max , AUC 0-inf ) of d-and l-amphetamine increased approximately three-fold from 10 mg to 30 mg indicating dose-proportional pharmacokinetics. The effect of food on the bioavailability of mixed salts of a single entity amphetamine product has not been studied. Metabolism and Excretion Amphetamine is reported to be oxidized at the 4 position of the benzene ring to form 4‑hydroxyamphetamine, or on the side chain α or β carbons to form alpha-hydroxy-amphetamine or norephedrine, respectively. Norephedrine and 4-hydroxy-amphetamine are both active and each is subsequently oxidized to form 4-hydroxy-norephedrine. Alpha-hydroxy-amphetamine undergoes deamination to form phenylacetone, which ultimately forms benzoic acid and its glucuronide and the glycine conjugate hippuric acid. Although the enzymes involved in amphetamine metabolism have not been clearly defined, CYP2D6 is known to be involved with formation of 4-hydroxy-amphetamine. Since CYP2D6 is genetically polymorphic, population variations in amphetamine metabolism are a possibility. Amphetamine is known to inhibit monoamine oxidase, whereas the ability of amphetamine and its metabolites to inhibit various P450 isozymes and other enzymes has not been adequately elucidated. In vitro experiments with human microsomes indicate minor inhibition of CYP2D6 by amphetamine and minor inhibition of CYP1A2, 2D6, and 3A4 by one or more metabolites. However, due to the probability of auto-inhibition and the lack of information on the concentration of these metabolites relative to in vivo concentrations, no predications regarding the potential for amphetamine or its metabolites to inhibit the metabolism of other drugs by CYP isozymes in vivo can be made. With normal urine pHs approximately half of an administered dose of amphetamine is recoverable in urine as derivatives of alpha-hydroxy-amphetamine and approximately another 30% to 40% of the dose is recoverable in urine as amphetamine itself. Since amphetamine has a pKa of 9.9, urinary recovery of amphetamine is highly dependent on pH and urine flow rates. Alkaline urine pHs result in less ionization and reduced renal elimination, and acidic pHs and high flow rates result in increased renal elimination with clearances greater than glomerular filtration rates, indicating the involvement of active secretion. Urinary recovery of amphetamine has been reported to range from 1% to 75%, depending on urinary pH, with the remaining fraction of the dose hepatically metabolized. Consequently, both hepatic and renal dysfunction have the potential to inhibit the elimination of amphetamine and result in prolonged exposures. In addition, drugs that affect urinary pH are known to alter the elimination of amphetamine, and any decrease in amphetamine’s metabolism that might occur due to drug interactions or genetic polymorphisms is more likely to be clinically significant when renal elimination is decreased (see PRECAUTIONS ).
A drug lookup is just the start. Eleplan keeps the whole care plan in one place.
Medications, diagnoses, documents, appointments, and the whole care team — organized and always in sync, with Ellie, your AI care assistant, on top of it. Free to start.