Medication reference
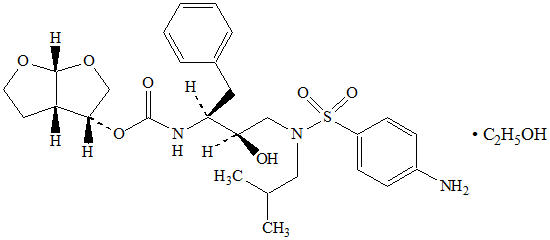
Darunavir
Protease Inhibitor [EPC] — ORAL
Darunavir — Protease Inhibitor [EPC]. INDICATIONS AND USAGE Darunavir tablets, co-administered with ritonavir (darunavir tablets/ritonavir), in combination with other antiretroviral agents
Boxed warning
BOXED WARNING
Brand names
DarunavirDarunavir 600 and 800 mgDARUNAVIRPREZISTA
Active ingredients
DARUNAVIRDARUNAVIR PROPYLENE GLYCOLATEDARUNAVIR HYDRATEDARUNAVIR ETHANOLATEDARUNAVIR DIHYDRATE
Indications
INDICATIONS AND USAGE Darunavir tablets, co-administered with ritonavir (darunavir tablets/ritonavir), in combination with other antiretroviral agents, is indicated for the treatment of human immunodeficiency virus (HIV-1) infection in adult and pediatric patients 3 years of age and older [see Use in Specific Populations (8.4) and Clinical Studies (14) ] . Darunavir tablets are a human immunodeficiency virus (HIV-1) protease inhibitor indicated for the treatment of HIV-1 infection in adult and pediatric patients 3 years of age and older. Darunavir tablets must be co-administered with ritonavir (darunavir tablets/ritonavir) and with other antiretroviral agents. (1)
Dosage
DOSAGE AND ADMINISTRATION Testing: In treatment-experienced patients, treatment history genotypic and/or phenotypic testing is recommended prior to initiation of therapy with darunavir/ritonavir to assess drug susceptibility of the HIV-1 virus ( 2.1 , 12.4 ) Monitor serum liver chemistry tests before and during therapy with darunavir/ritonavir. ( 2.1 , 2.2 , 5.2 ) Treatment-naïve adult patients and treatment-experienced adult patients with no darunavir resistance associated substitutions: 800 mg (one 800 mg tablet) taken with ritonavir 100 mg once daily and with food. ( 2.3 ) Treatment-experienced adult patients with at least one darunavir resistance associated substitution: 600 mg (one 600 mg tablet) taken with ritonavir 100 mg twice daily and with food. ( 2.3 ) Pregnant patients: 600 mg (one 600 mg tablet) taken with ritonavir 100 mg twice daily and with food. ( 2.4 ) Pediatric patients (3 to less than 18 years of age and weighing at least 10 kg): dosage of darunavir and ritonavir is based on body weight and should not exceed the adult dose. Darunavir should be taken with ritonavir and with food. ( 2.5 ) Darunavir/ritonavir is not recommended for use in patients with severe hepatic impairment. ( 2.6 ) 2.1 Testing Prior to Initiation of Darunavir/ritonavir In treatment-experienced patients, treatment history, genotypic and/or phenotypic testing is recommended to assess drug susceptibility of the HIV-1 virus [see Microbiology ( 12.4 )]. Refer to Dosage and Administration ( 2.3 ), ( 2.4 ) and ( 2.5 ) for dosing recommendations. Appropriate laboratory testing such as serum liver biochemistries should be conducted prior to initiating therapy with darunavir/ritonavir [see Warnings and Precautions ( 5.2 )]. 2.2 Monitoring During Treatment with Darunavir/ritonavir Patients with underlying chronic hepatitis, cirrhosis or in patients who have pre-treatment elevations of transaminases should be monitored for elevation in serum liver biochemistries, especially during the first several months of darunavir/ritonavir treatment [see Warnings and Precautions ( 5.2 )]. 2.3 Recommended Dosage in Adult Patients Darunavir must be co-administered with ritonavir to exert its therapeutic effect. Failure to correctly co-administer darunavir with ritonavir will result in plasma levels of darunavir that will be insufficient to achieve the desired antiviral effect and will alter some drug interactions. Patients who have difficulty swallowing darunavir tablets can use the 100 mg per mL darunavir oral suspension. Treatment-Naïve Adult Patients The recommended oral dose of darunavir is 800 mg (one 800 mg tablet or 8 mL of the oral suspension) taken with ritonavir 100 mg (one 100 mg tablet or capsule or 1.25 mL of a 80 mg per mL ritonavir oral solution) once daily and with food. An 8 mL darunavir dose should be taken as two 4 mL administrations with the included oral dosing syringe. Treatment-Experienced Adult Patients The recommended oral dosage for treatment-experienced adult patients is summarized in Table 1. Baseline genotypic testing is recommended for dose selection. However, when genotypic testing is not feasible, darunavir 600 mg taken with ritonavir 100 mg twice daily is recommended. Table 1 Recommended Darunavir/ritonavir Dosage in Treatment-Experienced Adult Patients a V11I, V32I, L33F, I47V, I50V, I54L, I54M, T74P, L76V, I84V and L89V b An 8 mL darunavir dose should be taken as two 4 mL administrations with the included oral dosing syringe Baseline Resistance Formulation and Recommended Dosing Darunavir tablets with ritonavir tablets or capsule Darunavir oral suspension (100 mg/mL) with ritonavir oral solution (80 mg/mL) With no darunavir resistance associated substitutions a One 800 mg darunavir tablet with one 100 mg ritonavir tablet/capsule, taken once daily with food 8 mL b darunavir oral suspension with 1.25 mL ritonavir oral solution, taken once daily with food With at least one darunavir resistance associated substitutions a , or with no baseline resistance information One 600 mg darunavir tablet with one 100 mg ritonavir tablet/capsule, taken twice daily with food 6 mL darunavir oral suspension with 1.25 mL ritonavir oral solution, taken twice daily with food 2.4 Recommended Dosage During Pregnancy The recommended dosage in pregnant patients is darunavir 600 mg taken with ritonavir 100 mg twice daily with food. Darunavir 800 mg taken with ritonavir 100 mg once daily should only be considered in certain pregnant patients who are already on a stable darunavir 800 mg with ritonavir 100 mg once daily regimen prior to pregnancy, are virologically suppressed (HIV-1 RNA less than 50 copies per mL) and in whom a change to twice daily darunavir 600 mg with ritonavir 100 mg may compromise tolerability or compliance. 2.5 Recommended Dosage in Pediatric Patients (age 3 to less than 18 years) Healthcare professionals should pay special attention to accurate dose selection of darunavir, transcription of the medication order, dispensing information and dosing instruction to minimize risk for medication errors, overdose and underdose. Prescribers should select the appropriate dose of darunavir/ritonavir for each individual child based on body weight (kg) and should not exceed the recommended dose for adults. Before prescribing darunavir, children weighing greater than or equal to 15 kg should be assessed for the ability to swallow tablets. If a child is unable to reliably swallow a tablet, the use of darunavir oral suspension should be considered. The recommended dose of darunavir/ritonavir for pediatric patients (3 to less than 18 years of age and weighing at least 10 kg is based on body weight (see Tables 2, 3, 4 and 5) and should not exceed the recommended adult dose. Darunavir should be taken with ritonavir and with food. The recommendations for the darunavir/ritonavir dosage regimens were based on pediatric clinical trial data and population pharmacokinetic modeling and simulation [see Use in Specific Populations ( 8.4 ) and Clinical Pharmacology ( 12.3 )]. Dosing Recommendations for Treatment-Naïve Pediatric Patients or Antiretroviral Treatment-Experienced Pediatric Patients with No Darunavir Resistance Associated Substitutions Pediatric Patients Weighing At Least 10 kg but Less than 15 kg The weight-based dose in antiretroviral treatment-naïve pediatric patients or antiretroviral treatment-experienced pediatric patients with no darunavir resistance associated substitutions is darunavir 35 mg/kg once daily with ritonavir 7 mg/kg once daily using the following table: Table 2 Recommended Dose for Pediatric Patients Weighing 10 kg to Less Than 15 kg Who are Treatment-Naïve or Treatment-Experienced with No Darunavir Resistance Associated Substitutions a a darunavir resistance associated substitutions: V11I, V32I, L33F, I47V, I50V, I54M, I54L, T74P, L76V, I84V and L89V b The 350 mg, 385 mg, 455 mg and 490 mg darunavir dose for the specified weight groups were rounded up for suspension dosing convenience to 3.6 mL, 4 mL, 4.6 mL and 5 mL, respectively. Body weight (kg) Formulation: Darunavir oral suspension (100 mg/mL) and ritonavir oral solution (80 mg/mL) Dose: once daily with food Greater than or equal to 10 kg to less than 11 kg Darunavir 3.6 mL b (350 mg) with ritonavir 0.8 mL (64 mg) Greater than or equal to 11 kg to less than 12 kg Darunavir 4 mL b (385 mg) with ritonavir 0.8 mL (64 mg) Greater than or equal to 12 kg to less than 13 kg Darunavir 4.2 mL (420 mg) with ritonavir 1 mL (80 mg) Greater than or equal to 13 kg to less than 14 kg Darunavir 4.6 mL b (455 mg) with ritonavir 1 mL (80 mg) Greater than or equal to 14 kg to less than 15 kg Darunavir 5 mL b (490 mg) with ritonavir 1.2 mL (96 mg) Pediatric Patients Weighing At Least 15 kg Pediatric patients weighing at least 15 kg can be dosed with darunavir oral tablet(s) using the following table: Table 3 Recommended Dose for Pediatric Patients Weighing At Least 15 kg Who are Treatment-Naïve or Treatment-Experienced
Warnings
WARNINGS AND PRECAUTIONS Drug-induced hepatitis (e.g., acute hepatitis, cytolytic hepatitis) has been reported with darunavir/ritonavir. Monitor liver function before and during therapy, especially in patients with underlying chronic hepatitis, cirrhosis or in patients who have pre-treatment elevations of transaminases. Post-marketing cases of liver injury, including some fatalities, have been reported. ( 5.2 ) Skin reactions ranging from mild to severe, including Stevens-Johnson Syndrome, toxic epidermal necrolysis, drug rash with eosinophilia and systemic symptoms and acute generalized exanthematous pustulosis, have been reported. Discontinue treatment if severe reaction develops. ( 5.3 ) Use with caution in patients with a known sulfonamide allergy. ( 5.4 ) Patients may develop new onset diabetes mellitus or hyperglycemia. Initiation or dose adjustments of insulin or oral hypoglycemic agents may be required. ( 5.6 ) Patients may develop redistribution/accumulation of body fat or immune reconstitution syndrome. ( 5.7 , 5.8 ) Patients with hemophilia may develop increased bleeding events. ( 5.9 ) Darunavir/ritonavir is not recommended in pediatric patients below 3 years of age in view of toxicity and mortality observed in juvenile rats dosed with darunavir up to days 23 to 26 of age. ( 5.10 ) 5.1 Importance of Co-administration with Ritonavir Darunavir must be co-administered with ritonavir and food to achieve the desired antiviral effect. Failure to administer darunavir with ritonavir and food may result in a loss of efficacy of darunavir. Please refer to ritonavir prescribing information for additional information on precautionary measures. 5.2 Hepatotoxicity Drug-induced hepatitis (e.g., acute hepatitis, cytolytic hepatitis) has been reported with darunavir/ritonavir. During the clinical development program (N=3,063), hepatitis was reported in 0.5% of patients receiving combination therapy with darunavir/ritonavir. Patients with pre-existing liver dysfunction, including chronic active hepatitis B or C, have an increased risk for liver function abnormalities including severe hepatic adverse events. Post-marketing cases of liver injury, including some fatalities, have been reported. These have generally occurred in patients with advanced HIV-1 disease taking multiple concomitant medications, having co-morbidities including hepatitis B or C co-infection and/or developing immune reconstitution syndrome. A causal relationship with darunavir/ritonavir therapy has not been established. Appropriate laboratory testing should be conducted prior to initiating therapy with darunavir/ritonavir and patients should be monitored during treatment. Increased AST/ALT monitoring should be considered in patients with underlying chronic hepatitis, cirrhosis or in patients who have pre-treatment elevations of transaminases, especially during the first several months of darunavir/ritonavir treatment. Evidence of new or worsening liver dysfunction (including clinically significant elevation of liver enzymes and/or symptoms such as fatigue, anorexia, nausea, jaundice, dark urine, liver tenderness, hepatomegaly) in patients on darunavir/ritonavir should prompt consideration of interruption or discontinuation of treatment. 5.3 Severe Skin Reactions During the clinical development program (n=3,063), severe skin reactions, accompanied by fever and/or elevations of transaminases in some cases, have been reported in 0.4% of subjects. Stevens-Johnson Syndrome was rarely (less than 0.1%) reported during the clinical development program. During post-marketing experience toxic epidermal necrolysis, drug rash with eosinophilia and systemic symptoms and acute generalized exanthematous pustulosis have been reported. Discontinue darunavir/ritonavir immediately if signs or symptoms of severe skin reactions develop. These can include but are not limited to severe rash or rash accompanied with fever, general malaise, fatigue, muscle or joint aches, blisters, oral lesions, conjunctivitis, hepatitis and/or eosinophilia. Rash (all grades, regardless of causality) occurred in 10.3% of subjects treated with darunavir/ritonavir [see Adverse Reactions ( 6 )] . Rash was mostly mild-to-moderate, often occurring within the first four weeks of treatment and resolving with continued dosing. The discontinuation rate due to rash in subjects using darunavir/ritonavir was 0.5%. Rash occurred more commonly in treatment-experienced subjects receiving regimens containing darunavir/ritonavir + raltegravir compared to subjects receiving darunavir/ritonavir without raltegravir or raltegravir without darunavir/ritonavir. However, rash that was considered drug related occurred at similar rates for all three groups. These rashes were mild to moderate in severity and did not limit therapy; there were no discontinuations due to rash. 5.4 Sulfa Allergy Darunavir contains a sulfonamide moiety. Darunavir should be used with caution in patients with a known sulfonamide allergy. In clinical studies with darunavir/ritonavir, the incidence and severity of rash were similar in subjects with or without a history of sulfonamide allergy. 5.5 Risk of Serious Adverse Reactions due to Drug Interactions Initiation of darunavir/ritonavir, a CYP3A inhibitor, in patients receiving medications metabolized by CYP3A or initiation of medications metabolized by CYP3A in patients already receiving darunavir/ritonavir, may increase plasma concentrations of medications metabolized by CYP3A and reduce plasma concentrations of active metabolite(s) formed by CYP3A. Initiation of medications that inhibit or induce CYP3A may increase or decrease concentrations of darunavir/ritonavir, respectively. These interactions may lead to: Clinically significant adverse reactions, potentially leading to severe, life threatening or fatal events from greater exposures of concomitant medications. Clinically significant adverse reactions from greater exposures of darunavir/ritonavir. Loss of therapeutic effect of the concomitant medications from lower exposures of active metabolite(s). Loss of therapeutic effect of darunavir/ritonavir and possible development of resistance from lower exposures of darunavir/ritonavir. See Table 10 for steps to prevent or manage these possible and known significant drug interactions, including dosing recommendations [see Drug Interactions ( 7 )]. Consider the potential for drug interactions prior to and during darunavir/ritonavir therapy; review concomitant medications during darunavir/ritonavir therapy; and monitor for the adverse reactions associated with the concomitant drugs [see Contraindications ( 4 ) and Drug Interactions ( 7 )]. 5.6 Diabetes Mellitus/Hyperglycemia New onset diabetes mellitus, exacerbation of pre-existing diabetes mellitus and hyperglycemia have been reported during postmarketing surveillance in HIV-infected patients receiving protease inhibitor (PI) therapy. Some patients required either initiation or dose adjustments of insulin or oral hypoglycemic agents for treatment of these events. In some cases, diabetic ketoacidosis has occurred. In those patients who discontinued PI therapy, hyperglycemia persisted in some cases. Because these events have been reported voluntarily during clinical practice, estimates of frequency cannot be made and causal relationships between PI therapy and these events have not been established. 5.7 Fat Redistribution Redistribution/accumulation of body fat, including central obesity, dorsocervical fat enlargement (buffalo hump), peripheral wasting, facial wasting, breast enlargement and "cushingoid appearance" have been observed in patients receiving antiretroviral therapy. The mechanism and long-term consequences of these events are currently unknown. A causal relationship has not been established. 5.8 Immune Reconstitution Syndrome Immune reconstitution syndrome has been reported in patients treated with combination antiretroviral therapy, including darunavir. During the in
Contraindications
CONTRAINDICATIONS Co-administration of darunavir tablets/ritonavir is contraindicated with drugs that are highly dependent on CYP3A for clearance and for which elevated plasma concentrations are associated with serious and/or life-threatening events (narrow therapeutic index). Examples of these drugs and othercontraindicated drugs (which may lead to reduced efficacy of darunavir) are listed below [see Drug Interactions (7.3) ] . Due to the need for co-administration of darunavir tablets with ritonavir, please refer to ritonavir prescribing information for a description of ritonavir contraindications. • Alpha 1-adrenoreceptor antagonist: alfuzosin • Anti-gout: colchicine, in patients with renal and/or hepatic impairment • Antimycobacterial: rifampin • Antipsychotics: lurasidone, pimozide • Cardiac Disorders: dronedarone, ivabradine, ranolazine • Ergot derivatives, e.g. dihydroergotamine, ergotamine, methylergonovine • Herbal product: St. John’s wort ( Hypericum perforatum ) • Hepatitis C direct acting antiviral: elbasvir/grazoprevir • Lipid modifying agents: lomitapide, lovastatin, simvastatin • Opioid Antagonist: naloxegol • PDE-5 inhibitor: sildenafil when used for treatment of pulmonary arterial hypertension • Sedatives/hypnotics: orally administered midazolam, triazolam • Co-administration of darunavir tablets/ritonavir is contraindicated with drugs that are highly dependent on CYP3A for clearance and for which elevated plasma concentrations are associated with serious and/or life-threatening events (narrow therapeutic index). ( 4 )
Drug interactions
DRUG INTERACTIONS Co-administration of darunavir/ritonavir with other drugs can alter the concentrations of other drugs and other drugs may alter the concentrations of darunavir. The potential drug-drug interactions must be considered prior to and during therapy. ( 4 , 5.5 , 7 , 12.3 ) 7.1 Potential for Darunavir/ritonavir to Affect Other Drugs Darunavir co-administered with ritonavir is an inhibitor of CYP3A, CYP2D6 and P-gp. Co-administration of darunavir and ritonavir with drugs that are primarily metabolized by CYP3A and CYP2D6 or are transported by P-gp may result in increased plasma concentrations of such drugs, which could increase or prolong their therapeutic effect and adverse events. Darunavir co-administered with ritonavir with drugs that have active metabolite(s) formed by CYP3A may result in reduced plasma concentrations of these active metabolite(s), potentially leading to loss of their therapeutic effect (see Table 10). 7.2 Potential for Other Drugs to Affect Darunavir Darunavir and ritonavir are metabolized by CYP3A. In vitro data indicate that darunavir may be a P-gp substrate. Drugs that induce CYP3A activity would be expected to increase the clearance of darunavir and ritonavir, resulting in lowered plasma concentrations of darunavir and ritonavir. Co-administration of darunavir and ritonavir and other drugs that inhibit CYP3A or P-gp may decrease the clearance of darunavir and ritonavir and may result in increased plasma concentrations of darunavir and ritonavir (see Table 10). 7.3 Established and Other Potentially Significant Drug Interactions Table 10 provides dosing recommendations as a result of drug interactions with darunavir/ritonavir. These recommendations are based on either drug interaction studies or predicted interactions due to the expected magnitude of interaction and potential for serious adverse events or loss of efficacy. The table includes examples of potentially significant interactions but is not all inclusive [see Contraindications ( 4 ) and Clinical Pharmacology ( 12.3 )] , and therefore the label of each drug that is co-administered with darunavir/ritonavir should be consulted for information related to the route of metabolism, interaction pathways, potential risks, and specific actions to be taken with regard to co-administration. Table 10 Established and Other Potentially Significant Drug Interactions: Alterations in Dose or Regimen May be Recommended Based on Drug Interaction Studies or Predicted Interaction (see Contraindications ( 4 ) for a list of examples of contraindicated drugs) [see Clinical Pharmacology ( 12.3 ) for Magnitude of Interaction, Tables 15 and 16] Concomitant Drug Class Drug Name Examples Effect on Concentration of Darunavir Or Concomitant Drug Clinical Comment HIV-1-Antiviral Agents: Nucleoside Reverse Transcriptase Inhibitors (NRTIs) didanosine ↔ darunavir ↔ didanosine Didanosine should be administered one hour before or two hours after darunavir/ritonavir (which are administered with food). HIV-1-Antiviral Agents: HIV-Protease Inhibitors (PIs) indinavir (The reference regimen for indinavir was indinavir/ritonavir 800/100 mg twice daily.) ↑ darunavir ↑ indinavir The appropriate dose of indinavir in combination with darunavir/ritonavir has not been established. lopinavir/ritonavir ↓ darunavir ↔ lopinavir Appropriate doses of the combination have not been established. Hence, it is not recommended to co-administer lopinavir/ritonavir and darunavir, with or without ritonavir. saquinavir ↓ darunavir ↔saquinavir Appropriate doses of the combination have not been established. Hence, it is not recommended to co-administer saquinavir and darunavir, with or without ritonavir. Other HIV protease inhibitors, except atazanavir [see Drug Interactions (7.4)] As co-administration with darunavir/ritonavir has not been studied, co-administration is not recommended. HIV-1-Antiviral Agents: CCR5 co-receptor antagonists maraviroc ↑ maraviroc When used in combination with darunavir/ritonavir, the dose of maraviroc should be 150 mg twice daily. Other Agents Alpha 1-adrenoreceptor antagonist: alfuzosin ↑ alfuzosin Co-administration is contraindicated due to potential for serious and/or life-threatening reactions such as hypotension. Antibacterial: clarithromycin ↔ darunavir ↑ clarithromycin No dose adjustment of the combination is required for patients with normal renal function. For co-administration of clarithromycin and darunavir/ritonavir in patients with renal impairment, the following dose adjustments should be considered: For subjects with CLcr of 30 mL/min to 60 mL/min, the dose of clarithromycin should be reduced by 50%. For subjects with CLcr of < 30 mL/min, the dose of clarithromycin should be reduced by 75%. Anticoagulants : Direct Oral Anticoagulants (DOACs) apixaban ↑ apixaban Due to potentially increased bleeding risk, dosing recommendations for co-administration of apixaban with darunavir/ritonavir depend on the apixaban dose. Refer to apixaban dosing instructions for co-administration with P-gp and strong CYP3A inhibitors in apixaban prescribing information. rivaroxaban ↑ rivaroxaban Co-administration of darunavir/ritonavir and rivaroxaban is not recommended because it may lead to an increased bleeding risk. dabigatran etexilate edoxaban ↑ dabigatran ↑ edoxaban Refer to the dabigatran etexilate or edoxaban prescribing information for recommendations regarding co-administration. The specific recommendations are based on indication, renal function, and effect of the co-administered P-gp inhibitors on the concentration of dabigatran or edoxaban. Clinical monitoring is recommended when a DOAC not affected by CYP3A4 but transported by P-gp, including dabigatran etexilate and edoxaban, is co-administered with darunavir /ritonavir. Other Anticoagulants warfarin ↓ warfarin ↔ darunavir Warfarin concentrations are decreased when co-administered with darunavir/ritonavir. It is recommended that the international normalized ratio (INR) be monitored when warfarin is combined with darunavir/ritonavir. Anticonvulsants: carbamazepine ↔ darunavir ↑ carbamazepine The dose of either darunavir/ritonavir or carbamazepine does not need to be adjusted when initiating co-administration with darunavir/ritonavir and carbamazepine. Clinical monitoring of carbamazepine concentrations and its dose titration is recommended to achieve the desired clinical response. clonazepam ↑ clonazepam Clinical monitoring of anticonvulsants that are metabolized by CYP3A is recommended. phenobarbital, phenytoin ↔ darunavir ↓ phenytoin ↓ phenobarbital Phenytoin and phenobarbital levels should be monitored when co-administering with darunavir/ritonavir. Antidepressants : Selective Serotonin Reuptake Inhibitors (SSRIs): paroxetine, sertraline ↓ paroxetine ↓ sertraline If either sertraline or paroxetine is initiated in patients receiving darunavir/ritonavir, dose titrating the SSRI based on a clinical assessment of antidepressant response is recommended. Monitor for antidepressant response in patients on a stable dose of sertraline or paroxetine who start treatment with darunavir/ritonavir. Tricyclic Antidepressants (TCAs): amitriptyline, desipramine, imipramine, nortriptyline ↑ amitriptyline ↑ desipramine ↑ imipramine ↑ nortriptyline Use a lower dose of the tricyclic antidepressants and trazodone due to potential increased adverse events such as nausea, dizziness, hypotension and syncope. Other: trazodone ↑ trazodone Antifungals: itraconazole, isavuconazole, ketoconazole, posaconazole ↑ darunavir ↑ itraconazole ↑ isavuconazole ↑ ketoconazole ↔ posaconazole Monitor for increased darunavir/ritonavir and/or antifungal adverse events with concomitant use of these antifungals. When co-administration is required, the daily dose of ketoconazole or itraconazole should not exceed 200 mg with monitoring for increased antifungal adverse events. voriconazole ↓ voriconazole Voriconazole is not recommended for patients receiving darunavir/ritonavir un
Adverse reactions
ADVERSE REACTIONS The following adverse reactions are discussed in other sections of labeling: Hepatotoxicity [see Warnings and Precautions ( 5.2 )] Severe Skin Reactions [see Warnings and Precautions ( 5.3 )] Diabetes Mellitus/Hyperglycemia [see Warnings and Precautions ( 5.6 )] Fat Redistribution [see Warnings and Precautions ( 5.7 )] Immune Reconstitution Syndrome [see Warnings and Precautions ( 5.8 )] Hemophilia [see Warnings and Precautions ( 5.9 )] Due to the need for co-administration of darunavir with ritonavir, please refer to ritonavir prescribing information for ritonavir-associated adverse reactions. The most common clinical adverse drug reactions to darunavir/ritonavir (incidence greater than or equal to 5%) of at least moderate intensity (greater than or equal to Grade 2) were diarrhea, nausea, rash, headache, abdominal pain and vomiting. ( 6 ) To report SUSPECTED ADVERSE REACTIONS, contact Viona Pharmaceuticals Inc. at 1-888-304-5011 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch. 6.1 Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice. Treatment Naïve-Adults: TMC114-C211 The safety assessment is based on all safety data from the Phase 3 trial TMC114-C211 comparing darunavir/ritonavir 800/100 mg once daily versus lopinavir/ritonavir 800/200 mg per day in 689 antiretroviral treatment-naïve HIV-1-infected adult subjects. The total mean exposure for subjects in the darunavir/ritonavir 800/100 mg once daily arm and in the lopinavir/ritonavir 800/200 mg per day arm was 162.5 and 153.5 weeks, respectively. The majority of the adverse drug reactions (ADRs) reported during treatment with darunavir/ritonavir 800/100 mg once daily were mild in severity. The most common clinical ADRs to darunavir/ritonavir 800/100 mg once daily (greater than or equal to 5%) of at least moderate intensity (greater than or equal to Grade 2) were diarrhea, headache, abdominal pain and rash. 2.3% of subjects in the darunavir/ritonavir arm discontinued treatment due to ADRs. ADRs to darunavir/ritonavir 800/100 mg once daily of at least moderate intensity (greater than or equal to Grade 2) in antiretroviral treatment-naïve HIV-1-infected adult subjects are presented in Table 6 and subsequent text below the table. Table 6 Selected Clinical Adverse Drug Reactions to Darunavir/ritonavir 800/100 mg Once Daily a of at Least Moderate Intensity (≥ Grade 2) Occurring in ≥ 2% of Antiretroviral Treatment-Naïve HIV-1-Infected Adult Subjects (Trial TMC114-C211) N=total number of subjects per treatment group; FTC=emtricitabine; TDF=tenofovir disoproxil fumarate a Excluding laboratory abnormalities reported as ADRs. System organ class, preferred term, % Darunavir/ritonavir 800/100 mg once daily + TDF/FTC N=343 Lopinavir/ritonavir 800/200 mg per day + TDF/FTC N=346 Gastrointestinal Disorders Abdominal pain 6% 6% Diarrhea 9% 16% Nausea 4% 4% Vomiting 2% 4% General Disorders and Administration Site Conditions Fatigue < 1% 3% Metabolism and Nutrition Disorders Anorexia 2% < 1% Nervous System Disorders Headache 7% 6% Skin and Subcutaneous Tissue Disorders Rash 6% 7% Less Common Adverse Reactions Treatment-emergent ADRs of at least moderate intensity (greater than or equal to Grade 2) occurring in less than 2% of antiretroviral treatment-naïve subjects receiving darunavir/ritonavir 800/100 mg once daily are listed below by body system: Gastrointestinal Disorders : acute pancreatitis, dyspepsia, flatulence General Disorders and Administration Site Conditions : asthenia Hepatobiliary Disorders : acute hepatitis (e.g., acute hepatitis, cytolytic hepatitis, hepatotoxicity) Immune System Disorders : (drug) hypersensitivity, immune reconstitution syndrome Metabolism and Nutrition Disorders : diabetes mellitus Musculoskeletal and Connective Tissue Disorders : myalgia, osteonecrosis Psychiatric Disorders : abnormal dreams Skin and Subcutaneous Tissue Disorders : angioedema, pruritus, Stevens-Johnson Syndrome, urticaria Laboratory Abnormalities Selected Grade 2 to 4 laboratory abnormalities that represent a worsening from baseline observed in antiretroviral treatment-naïve adult subjects treated with darunavir/ritonavir 800/100 mg once daily are presented in Table 7. Table 7 Grade 2 to 4 Laboratory Abnormalities Observed in Antiretroviral Treatment-Naïve HIV-1-Infected Adult Subjects a (Trial TMC114-C211) N=total number of subjects per treatment group; FTC=emtricitabine; TDF=tenofovir disoproxil fumarate a Grade 4 data not applicable in Division of AIDS grading scale. Laboratory parameter % Limit Darunavir /ritonavir 800/100 mg once daily + TDF/FTC Lopinavir/ ritonavir 800/200 mg per day + TDF/FTC Biochemistry Alanine Aminotransferase Grade 2 > 2.5 to ≤ 5 X ULN 9% 9% Grade 3 > 5 to ≤ 10 X ULN 3% 3% Grade 4 > 10 X ULN < 1% 3% Aspartate Aminotransferase Grade 2 > 2.5 to ≤ 5 X ULN 7% 10% Grade 3 > 5 to ≤ 10 X ULN 4% 2% Grade 4 > 10 X ULN 1% 3% Alkaline Phosphatase Grade 2 > 2.5 to ≤ 5 X ULN 1% 1% Grade 3 > 5 to ≤ 10 X ULN 0% < 1% Grade 4 > 10 X ULN 0% 0% Hyperbilirubinemia Grade 2 > 1.5 to ≤ 2.5 X ULN < 1% 5% Grade 3 > 2.5 to ≤ 5 X ULN < 1% < 1% Grade 4 > 5 X ULN 0% 0% Triglycerides Grade 2 5.65 mmol/L to 8.48 mmol/L 500 mg/dL to 750 mg/dL 3% 10% Grade 3 8.49 mmol/L to 13.56 mmol/L 751 mg/dL to 1,200 mg/dL 2% 5% Grade 4 > 13.56 mmol/L > 1,200 mg/dL 1% 1% Total Cholesterol Grade 2 6.20 mmol/L to 7.77 mmol/L 240 mg/dL to 300 mg/dL 23% 27% Grade 3 > 7.77 mmol/L > 300 mg/dL 1% 5% Low-Density Lipoprotein Cholesterol Grade 2 4.13 mmol/L to 4.90 mmol/L 160 mg/dL to 190 mg/dL 14% 12% Grade 3 ≥ 4.91 mmol/L ≥ 191 mg/dL 9% 6% Elevated Glucose Levels Grade 2 6.95 mmol/L to 13.88 mmol/L 126 mg/dL to 250 mg/dL 11% 10% Grade 3 13.89 mmol/L to 27.75 mmol/L 251 mg/dL to 500 mg/dL 1% < 1% Grade 4 > 27.75 mmol/L > 500 mg/dL 0% 0% Pancreatic Lipase Grade 2 > 1.5 to ≤ 3 X ULN 3% 2% Grade 3 > 3 to ≤ 5 X ULN < 1% 1% Grade 4 > 5 X ULN 0% < 1% Pancreatic Amylase Grade 2 > 1.5 to ≤ 2 X ULN 5% 2% Grade 3 > 2 to ≤ 5 X ULN 5% 4% Grade 4 > 5 X ULN 0% < 1% Treatment-Experienced Adults: TMC114-C214 The safety assessment is based on all safety data from the Phase 3 trial TMC114-C214 comparing darunavir/ritonavir 600/100 mg twice daily versus lopinavir/ritonavir 400/100 mg twice daily in 595 antiretroviral treatment-experienced HIV-1-infected adult subjects. The total mean exposure for subjects in the darunavir/ritonavir 600/100 mg twice daily arm and in the lopinavir/ritonavir 400/100 mg twice daily arm was 80.7 and 76.4 weeks, respectively. The majority of the ADRs reported during treatment with darunavir/ritonavir 600/100 mg twice daily were mild in severity. The most common clinical ADRs to darunavir/ritonavir 600/100 mg twice daily (greater than or equal to 5%) of at least moderate intensity (greater than or equal to Grade 2) were diarrhea, nausea, rash, abdominal pain and vomiting. 4.7% of subjects in the darunavir/ritonavir arm discontinued treatment due to ADRs. ADRs to darunavir/ritonavir 600/100 mg twice daily of at least moderate intensity (greater than or equal to Grade 2) in antiretroviral treatment-experienced HIV-1-infected adult subjects are presented in Table 8 and subsequent text below the table. Table 8 Selected Clinical Adverse Drug Reactions to Darunavir/ritonavir 600/100 mg Twice Daily a of at Least Moderate Intensity (≥ Grade 2) Occurring in ≥ 2% of Antiretroviral Treatment-Experienced HIV-1-Infected Adult Subjects (Trial TMC114-C214) N=total number of subjects per treatment group; OBR=optimized background regimen a Excluding laboratory abnormalities reported as ADRs System organ class, preferred term, % Darunavir/ritonavir 600/100 mg twice daily + OBR N=298 Lopinavir/ritonavir 400/100 mg twice daily + OBR N=297 Gastrointestinal Disorders Abdominal distension 2% <
Mechanism of action
Mechanism of Action Darunavir is an HIV-1 antiviral drug [see Microbiology (12.4) ] . Mechanism of Action Darunavir is an inhibitor of the HIV-1 protease. It selectively inhibits the cleavage of HIV-1 encoded Gag-Pol polyproteins in infected cells, thereby preventing the formation of mature virus particles.
Available forms (12)
darunavir 100 MG/ML Oral Suspensiondarunavir 150 MG Oral Tabletdarunavir 300 MG Oral Tabletdarunavir 400 MG Oral Tabletdarunavir 600 MG Oral Tabletdarunavir 75 MG Oral Tabletdarunavir 800 MG Oral Tabletdarunavir 100 MG/ML Oral Suspension [Prezista]branddarunavir 150 MG Oral Tablet [Prezista]branddarunavir 600 MG Oral Tablet [Prezista]branddarunavir 75 MG Oral Tablet [Prezista]branddarunavir 800 MG Oral Tablet [Prezista]brand
NDC examples
72578-14772578-14868071-391031722-08831722-08969097-24469097-24868180-34568180-34660687-80860687-81931722-567
Indicated ICD-10 codes
Treats these conditions
Assistance programs
AIDS Drug Assistance Program (ADAP)AIDS Education and Training Centers (AETC) ProgramCoordinated Services and Access to Research for Women, Infants, Children, and YouthEnding the HIV Epidemic: A Plan for America — Ryan White HIV/AIDS Program Parts A and BGrants to Provide Outpatient Early Intervention Services with Respect to HIV DiseaseHIV Care Formula GrantsHIV Emergency Relief Project GrantsHIV-Related Training and Technical AssistanceHousing Opportunities for Persons with AIDSSpecial Projects of National Significance
Source: openFDA + RxNorm · 2026
Look up another medication